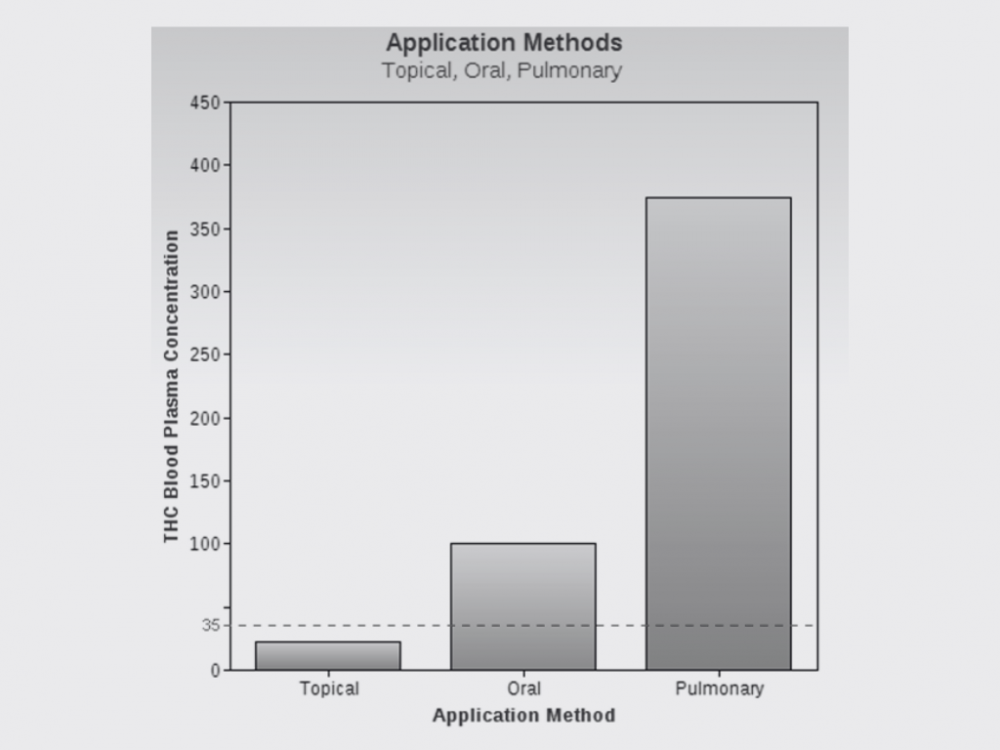
Application method vs THC plasma concentration: topical, oral, pulmonary
THC Plasma Concentrations: A Comparison Across Application Methods
Introduction
Tetrahydrocannabinol (THC), one of the most well-studied cannabinoids, has a range of physiological effects mediated through its binding to CB1 and CB2 receptors in the endocannabinoid system. The pharmacokinetics of THC, including its concentration in the bloodstream, can vary significantly depending on the route of administration—be it topical, oral, or pulmonary. This article elaborates on the anticipated THC blood concentrations resulting from different application methods.
Topical Administration
When applied topically, THC primarily interacts with local cannabinoid receptors and is minimally absorbed into the bloodstream. Hence, topical applications typically result in negligible systemic THC concentrations. This method is often preferred for localized relief, such as treating skin conditions or localized pain (Huestis, 2007).
Oral/Ingestion Administration
Oral administration of THC, commonly via edibles or tinctures, leads to its first-pass metabolism in the liver. This process produces metabolites like 11-hydroxy-THC, which can be more potent than THC itself. Peak blood concentrations can occur 1-6 hours post-ingestion, with lower bioavailability ranging from 4-20% due to factors like metabolism and fat solubility (Grotenhermen, 2003; Ohlsson et al., 1980).
Pulmonary/Inhalational Administration
Inhalation methods, such as smoking or vaporizing, provide the most rapid onset of effects, usually within minutes. Pulmonary administration avoids first-pass metabolism, leading to higher bioavailability (about 30%) and peak plasma concentrations within 3-10 minutes post-inhalation (Huestis, 2007; Newmeyer et al., 2017).
Comparative Analysis
While topical use generally leads to minimal systemic absorption, pulmonary methods result in the most rapid and significant increase in THC blood concentrations. Oral ingestion sits in between, characterized by delayed but sometimes more prolonged and potentially potent effects due to metabolite formation (Spindle et al., 2019).
Special Medical Considerations
Individuals with the following medical conditions should exercise caution when considering cannabinoid therapies:
Respiratory Disorders
Liver Diseases
Cardiovascular Conditions
Pregnancy and Breastfeeding
Mental Health Disorders
For such cases, consulting Dr. Benjamin Caplan at CED Clinic is advised for guided, evidence-based treatment plans.
References
Huestis, M. A. (2007). Human Cannabinoid Pharmacokinetics. Chemistry & Biodiversity, 4(8), 1770-1804.
Grotenhermen, F. (2003). Pharmacokinetics and pharmacodynamics of cannabinoids. Clinical Pharmacokinetics, 42(4), 327-360.
Ohlsson, A., Lindgren, J. E., Wahlen, A., Agurell, S., Hollister, L. E., & Gillespie, H. K. (1980). Plasma delta-9-tetrahydrocannabinol concentrations and clinical effects after oral and intravenous administration and smoking. Clinical Pharmacology and Therapeutics, 28(3), 409-416.
Newmeyer, M. N., Swortwood, M. J., Abulseoud, O. A., & Huestis, M. A. (2017). Subjective and physiological effects, and expired carbon monoxide concentrations in frequent and occasional cannabis smokers following smoked, vaporized, and oral cannabis administration. Drug and Alcohol Dependence, 175, 67-76.
Spindle, T. R., Cone, E. J., Schlienz, N. J., Mitchell, J. M., Bigelow, G. E., Flegel, R., … & Vandrey, R. (2019). Acute Effects of Smoked and Vaporized Cannabis in Healthy Adults Who Infrequently Use Cannabis: A Crossover Trial. JAMA Network Open, 2(11), e1917458.
Contact Dr. Benjamin Caplan at CED Clinic for specialized guidance in cannabinoid therapies, especially if you have specific medical conditions that necessitate careful treatment planning. Dr. Caplan offers expert advice tailored to individual health profiles and needs.
Delving into THC Application Methods and Their Impact on Plasma Concentration
The way tetrahydrocannabinol (THC) is administered plays a significant role in its absorption, bioavailability, and ultimately, its concentration in the plasma. A detailed comparison of topical, oral, and pulmonary methods reveals distinct pharmacokinetic profiles that influence both the therapeutic efficacy and safety of THC use.
Topical application of THC provides localized effects with minimal systemic absorption, making it a preferred option for targeted relief without psychoactive outcomes. However, the plasma levels of THC achieved through this method are significantly lower than those resulting from oral or pulmonary routes, given the skin’s limited permeability to cannabinoids.
Oral consumption of THC, such as through edibles or capsules, is characterized by a delayed onset of effects due to the digestion process and first-pass metabolism in the liver. This route tends to produce variable plasma concentrations of THC, with peak levels occurring several hours after ingestion. The bioavailability of THC via oral administration is generally lower compared to inhalation but results in longer-lasting effects.
Pulmonary administration, including smoking and vaping, allows for rapid absorption of THC directly into the bloodstream through the lungs, leading to quicker onset times and higher peak plasma concentrations. This method is often preferred for immediate relief, though it requires careful dose management to avoid potential adverse effects.
The choice of application method impacts not only the plasma concentration of THC but also its therapeutic outcomes and safety profile. Factors such as the individual’s metabolism, the presence of other cannabinoids and terpenes, and specific health conditions can further influence THC’s pharmacokinetics.
Understanding the pharmacodynamics of THC across different application methods is crucial for optimizing treatment regimens, especially in medical cannabis use. Clinical trials and patient-reported outcomes continue to provide valuable insights into the efficacy and safety of various THC administration routes.
As cannabis research progresses, innovations in delivery systems aim to improve the bioavailability and predictability of THC effects, tailored to individual needs and preferences. Future directions in this field will likely focus on developing more sophisticated formulations and technologies to enhance the therapeutic potential of THC while minimizing adverse outcomes.
Educating both patients and healthcare providers on the nuances of THC application methods is essential for informed decision-making, ensuring that cannabis use is both effective and aligned with the individual’s therapeutic goals.