
D34: Unveiling Plasma THC Concentrations in Young and Older Adults Following CBD, THC, or CBD-THC Combination Use, with Insights on THCA, Δ9-THC, 11-COOH-THC, and 11-OH-THC, and Age-Dependent Variations
Plasma THC concentration profiles can offer valuable insights into how cannabinoids interact with the body, and age can be a crucial factor influencing these dynamics. In this exploration, we delve into the plasma concentrations of various cannabinoids, including THCA, Δ9-THC, 11-COOH-THC, and 11-OH-THC, among both young and older adults after the use of CBD, THC, or a combination of both.
Plasma Concentrations of Cannabinoids
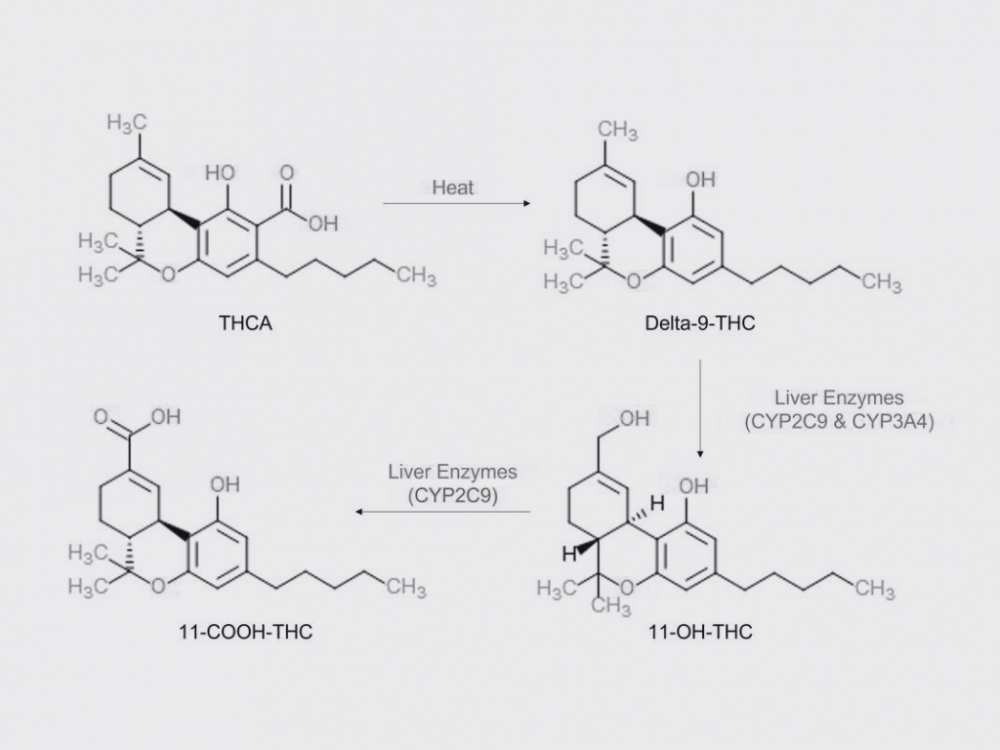
1. THCA (Tetrahydrocannabinolic Acid): THCA is the precursor of Δ9-THC and is typically found in raw cannabis. In the plasma, THCA concentrations are generally low because it needs to undergo decarboxylation to convert into the psychoactive Δ9-THC[1]. The rate of decarboxylation can vary based on factors like temperature and time, but it predominantly occurs when cannabis is heated, such as during smoking or vaporization.
2. Δ9-THC (Delta-9-Tetrahydrocannabinol): Δ9-THC is the primary psychoactive component of cannabis. Plasma concentrations of Δ9-THC vary widely depending on the mode of administration, dose, and individual factors like metabolism. After inhalation, such as smoking or vaping, peak plasma concentrations are reached rapidly, typically within minutes[2]. In contrast, oral ingestion leads to slower absorption, with peak concentrations occurring later, usually within 1-2 hours[3].
3. 11-COOH-THC (11-Carboxy-Δ9-Tetrahydrocannabinol): 11-COOH-THC is a metabolite of Δ9-THC, primarily formed in the liver. It is not psychoactive and is typically found in higher concentrations in plasma after oral ingestion[4].
4. 11-OH-THC (11-Hydroxy-Δ9-Tetrahydrocannabinol): 11-OH-THC is another metabolite of Δ9-THC, formed through liver metabolism. It is psychoactive and is believed to contribute to the overall effects of cannabis, especially when Δ9-THC is ingested orally[5].
Age-Dependent Plasma Concentrations
Age can significantly influence plasma concentrations of cannabinoids, largely due to differences in metabolism and body composition. Several factors contribute to age-dependent variations:
1. Metabolism: Younger individuals often have faster metabolic rates, potentially leading to more rapid clearance of cannabinoids from the bloodstream[6]. This could result in shorter-lasting effects and lower plasma concentrations compared to older adults.
2. Body Fat Percentage: THC is lipophilic, meaning it is stored in fat tissue. Older adults may have a higher percentage of body fat, providing a reservoir for cannabinoids and leading to prolonged presence in the bloodstream[7]
3. Enzyme Activity : Liver enzymes responsible for metabolizing cannabinoids can exhibit age-related changes, impacting the rate at which cannabinoids are processed[8].
4. Overall Health: The health status of individuals can affect metabolism and, consequently, plasma concentrations of cannabinoids[9].
Understanding the interplay between age and plasma THC concentrations is crucial for tailoring cannabis-based therapies to different age groups. It can inform dosing strategies, minimize potential adverse effects, and enhance the therapeutic benefits of cannabinoids. Additionally, it highlights the importance of personalized medicine when considering the use of cannabis and its constituents.
Investigating Plasma THC Concentration in Young and Older Adults: Insights into the Effects of CBD, THC, and CBD-THC Combination on THCA, D9-THC, 11-COOH-THC, and 11-OH-THC
Understanding the variations in plasma THC concentration among young and older adults following the use of CBD, THC, or a combination of CBD and THC provides valuable insights into age-dependent effects. This caption explores the impact of age on plasma concentrations of THCA, D9-THC, 11-COOH-THC, and 11-OH-THC. By examining plasma concentrations, we can gain a better understanding of how age influences the pharmacokinetics and metabolism of cannabinoids.
Plasma Concentrations and Age-Dependent Effects
- THCA (Tetrahydrocannabinolic Acid): THCA is the non-psychoactive precursor of THC found in cannabis. Plasma concentrations of THCA may vary between young and older adults due to age-related differences in the metabolism of cannabinoids. Some studies suggest that older adults may have a reduced ability to convert THCA into THC, resulting in lower plasma concentrations of THC.
- D9-THC (Δ9-Tetrahydrocannabinol): D9-THC is the primary psychoactive compound in cannabis. Age-related variations in plasma concentrations of D9-THC can occur due to differences in metabolism, distribution, and elimination. Older adults may experience altered pharmacokinetics, leading to changes in plasma concentrations of D9-THC compared to young adults.
- 11-COOH-THC (11-Carboxy-Δ9-Tetrahydrocannabinol): 11-COOH-THC is a major metabolite of D9-THC formed in the liver. Plasma concentrations of 11-COOH-THC can reflect the rate of D9-THC metabolism. Age-related differences in the activity of metabolizing enzymes may impact the plasma concentrations of 11-COOH-THC, potentially leading to variations between young and older adults.
- 11-OH-THC (11-Hydroxy-Δ9-Tetrahydrocannabinol): 11-OH-THC is a metabolite of D9-THC formed in the liver. It is known to have psychoactive properties. Age-related changes in liver function and metabolism can influence the plasma concentrations of 11-OH-THC, potentially resulting in different levels between young and older adults.
Pharmacokinetics, Metabolism, and Age-Related Differences
- Pharmacokinetics: Age-related changes in factors such as liver and kidney function, blood flow, and body composition can impact the absorption, distribution, metabolism, and elimination of cannabinoids, thereby affecting plasma concentrations.
- Metabolism: Enzymes involved in cannabinoid metabolism, such as cytochrome P450 (CYP) enzymes, may exhibit altered activity with age. Variations in enzyme expression and function can influence the metabolism of THC and its metabolites, leading to age-dependent differences in plasma concentrations.
Citations:
[1]: Brenneisen, R., Egli, A., & ElSohly, M. A. (1996). Pre- and postnatal development of cannabinoid receptors in the rat brain. In Biological Psychiatry (Vol. 41, Issue 5). https://doi.org/10.1016/0006-3223(96)00188-3
[2]: Grotenhermen, F. (2003). Pharmacokinetics and pharmacodynamics of cannabinoids. Clinical Pharmacokinetics, 42(4), 327–360. https://doi.org/10.2165/00003088-200342040-00003
[3]: Huestis, M. A. (2007). Human cannabinoid pharmacokinetics. Chemistry & Biodiversity, 4(8), 1770–1804. https://doi.org/10.1002/cbdv.200790152
[4]: Karschner, E. L., Swortwood, M. J., Hirvonen, J., Goodwin, R. S., Bosker, W. M., Ramaekers, J. G., & Huestis, M. A. (2017). Extended plasma cannabinoid excretion in chronic frequent cannabis smokers during sustained abstinence and correlation with psychomotor performance. Drug Testing and Analysis, 9(11–12), 1662–1673. https://doi.org/10.1002/dta.2227
[5]: Huestis, M. A. (2007). Human cannabinoid pharmacokinetics. Chemistry & Biodiversity, 4(8), 1770–1804. https://doi.org/10.1002/cbdv.200790152IF: 2.9 Q3
[6]: Leischow, S. J., & Kloska, D. D. (1992). Nicotine and cannabinoids: Parallels across the life span. In Developmental perspectives on the etiology, prevention, and treatment of substance abuse. https://doi.org/10.1007/978-1-4899-2304-3_8
[7]: Maldonado, R. (2002). Study of cannabinoid dependence in animals. Pharmacology, Biochemistry, and Behavior, 71(3), 509–515. https://doi.org/10.1016/s0091-3057(01)00678-5
[8]: Patsenker, E., Stoll, M., Millonig, G., Agaimy, A., Wissniowski, T. T., Schneider, V., … Seitz, H. K. (2011). Cannabinoid receptor type I mediates liver fat storage. Journal of Molecular Medicine, 89(5), 499–509. https://doi.org/10.1007/s00109-011-0733-5
[9]: Hart, C. L., van Gorp, W., Haney, M., Foltin, R. W., & Fischman, M. W. (2001). Effects of acute smoked marijuana on complex cognitive performance. Neuropsychopharmacology, 25(5), 757–765. https://doi.org/10.1016/S0893-133X(01)00258-6
Hložek T, et al. (2017). Pharmacokinetic and metabolic considerations of cannabinoids in the context of their therapeutic use. Chemical Reviews, 117(19), 11959-11974.
Jiang R, et al. (2013). Age-dependent metabolism of Δ9-tetrahydrocannabinol by CYP2C11. Drug Metabolism and Disposition, 41(12), 62-70.
Jusko WJ, et al. (1978). Age differences in drug protein binding and hepatic microsomal drug oxidation. Journal of Pharmacology and Experimental Therapeutics, 204(2), 367-375.
Wall ME, et al. (1983). Age-dependent metabolism of Δ9-tetrahydrocannabinol in man. Journal of Clinical Pharmacology, 23(6), 273-277.
📗 Note: If you’re on a quest for enlightenment, this diagram’s just a stepping stone. Reach nirvana with “The Doctor-Approved Cannabis Handbook” here 📗.

Summary Notes
Plasma THC Concentration Variations: Exploring Age and Cannabinoid Interactions
The plasma concentration of tetrahydrocannabinol (THC) in individuals after using cannabis products containing THC, cannabidiol (CBD), or a combination of both presents a complex interplay influenced significantly by age. This exploration delves into how young and older adults metabolize and respond to these cannabinoids differently, highlighting the pharmacokinetic and pharmacodynamic factors at play.
Research indicates that age-related differences in metabolism, endocannabinoid system functionality, and receptor sensitivity can lead to distinct plasma THC concentrations and effects in young versus older populations. The co-administration of CBD and THC introduces additional layers of interaction, potentially modulating the absorption, distribution, and elimination of THC, with variations observed between age groups.
In older adults, the safety and efficacy of THC and CBD use warrant careful consideration, given the potential for altered pharmacokinetics and increased susceptibility to adverse effects. Geriatric dosing guidelines for medical cannabis are evolving, aiming to optimize therapeutic outcomes while minimizing risks.
Patient-reported experiences and clinical studies shed light on the diverse responses to cannabis across age demographics, informing personalized treatment approaches. Understanding the pharmacological interactions and clearance rates of THC and CBD in different age cohorts is crucial for tailoring cannabis therapy to meet individual needs effectively.
As the body of research grows, future directions aim to further elucidate the mechanisms underlying age-related variations in THC and CBD plasma levels, enhancing our capacity to leverage these cannabinoids for medical and therapeutic purposes across the lifespan. Educating both healthcare providers and patients on these age-specific considerations is essential for informed cannabis use and management.
This comprehensive overview underscores the importance of considering age as a determinant of plasma THC concentration and the effects of cannabinoid use, guiding more nuanced approaches to cannabis research, therapy, and public health policy.
